

Calibrating a semi-adjustable articulator
Martin McKinstry is a dental surgeon at Langlands Road Dental Care in Glasgow. He graduated in 2006, with MJDF and MRCPS, and has been a practice owner since 2019. Martin has an interst in orthodontics, implants, digital dentistry and cosmetic restorations. Here he discusses the use of a semi-adjustable articulator and details the essential process of calibrating the device
So, all of us general dental practitioners understand the importance of the semi-adjustable articulator in restorative dentistry and we use them routinely for all indirect fixed prosthodontic cases, right? No? Until recently, neither did I.
We have all had cases where we expect the fitting of a crown to be a straightforward job only to spend 20 minutes grinding the occlusal surface because it is high. Typically, we assess our patients’ static occlusion and fail to take the dynamic occlusion into account. Frequently, the result is that a crown looks great on the study models but doesn’t seem to fit in real life. We usually get away with it to a large extent too.
As stated by Davies, Gray and Qualtrough (2002): ‘There is no such thing as an intrinsically bad occlusal contact, only an intolerable number of times to (para)function on it’. But simply getting away with is hardly good practice and is definitely not what we should be striving for as professionals.
It becomes exponentially more difficult to get away with it when we start proving more complex treatments such as multiple-unit bridges, implant-borne restorations or full-arch rehabilitations.
The articulatory system
The articulatory system has been likened to a tripod, with the teeth being one leg and the temporomandibular joints being the other two.
The semi-adjustable articulator allows the mounting of study and working casts with the hinge representing a reasonable approximation of the anatomical position of the patient’s TMJ. Having defined the spatial relationship of the tripod legs, the articulating condyle of the articulator simulates the movements of the TMJ, allowing us to assess and confirm to the patient’s dynamic occlusion.
But this is like any other machine. It requires maintenance and calibration: the larger the number of working parts, the more there is to go wrong. The more it’s used, the more it will be subject to wear and tear, accidental damage and decreasing accuracy. This shouldn’t be a problem if the same articulator is used each time a given set of casts is mounted.
In a commercial lab however, if models are mounted on one articulator, then another is used in construction of a restoration, inaccuracies can creep in, potentially affecting the final result.
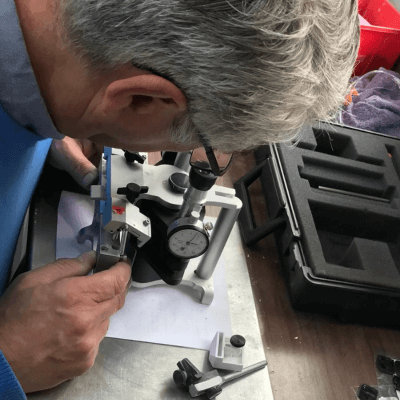
The gold standard is the periodic calibration of articulators using a calibration gauge to eliminate any discrepancy. Denar produces a gauge that fits onto the upper member of the articulator, with eyepieces that allow visualisation into the condylar element. Corrections are carefully made using the adjustment screws on the articulator until the crosshairs on the condylar elements line up with the crosshairs in
the eyepieces of the calibration gauge.
In action
Students at the University of Manchester’s MSc course in advanced restorative dentistry were recently lucky enough to be able to watch the procedure being carried out by head dental technician Stephen Ford. The increments on the gauge are a miniscule 0.0005 inches, representing an incredibly high degree of accuracy. While the calibration gauge is likely unnecessary for the GDP, it is advisable for commercial labs to have one available.
In addition to regularly calibrating their own articulators, labs could offer a calibration service for dentists’ articulators. The result would be a more standardised process with elimination of a source of errors in order to keep our patients comfortable and happy.
This article was originally published in Clinical Dentistry, September 2023.
Product used Denar Mark II Articulator, supplied by Prestige Dental. This company also provides a specialist repair and re-calibration service for articulators, for more information contact Paul Martin, paul@prestige-dental.co.uk or 01274 721567.
MSc Advanced Restorative Dentistry For more details about the University of Manchester MSc advanced restorative dentistry course, email Professor Hugh Devlin, the academic lead of the programme at hugh.devlin@manchester.ac.uk
Reference: Davies, Gray, Qualtrough (2002) Management of tooth surface loss BR Dent/192(1) 11.23



Copyright © Prestige Dental Products UK Ltd 2026
Registered in England, UK no. 2391338. VAT no. 5580015.